Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Case Report - (2015) Volume 0, Issue 0
;
Background: High grade fever and atypical pneumonia in a susceptible Asian epidemic area could construe fatal consequences attributable to specific prevalence factitious organism: i.e Bukholderia pseudomallei.
Case report: A 59 years old Indonesian man with predisposing factors of meliodosis initially presented with acuteshortness of breath and severe frontal headache associated in Emergency Department of Hospital Teluk Intan,Malaysia. He had history of prolonged low grade fever and non-productive cough for 5 days.
Methods/Results: Culture and sensitivity test for blood and pleural fluid were negative for pathogenic organism.The specific tests for tuberculosis were non-reactive for Tuberculos bacilli. The specific oxidase-negative culture and sensitivity for psedomonas was positive after day 3 of hospitalisation and the IGM-ELISA titre antibody level for meliodosis was positive. The patient was well responded to immediate treatment and was discharged for a regular outpatient follow-up for eradication therapy.
Conclusion: This case report documents the potential symptoms associated with atypical pneumonia in recognising Meliodosis in an epidemic Asian area. Early suspicion may avert untowards fatal consequences and improved the quality of life.
Keywords: Fever; Cough; Melioidosis; Atypical pneumonia; Malaysia; Epidemic; Asian
Melioidosis, caused by the environmental gram negative bacillus Bukholderia pseudomallei, is classically characterized by pneumonia and multiple abscess [1]. Its diagnosis is rather is challenging as its clinical symptomatology is varied and requires specific culture medium for isolation of the pathogen. It is important to detect it early and excluding it from the common pneumonial infection presentation as it may cause severe complications and fatal, with a mortality rate up to 40% in epidemic Asia area and 65% septicaemic form in 1980s in Malaysia [2,3]. Eradication of the organism following infection is difficult with a slow fever-clearance time, the need for prolonged antibiotic therapy and a high rate of relapse if the therapy is incomplete. This case report documents the potential of detecting a suspicious symptoms associated with atypical pneumonia in recognising Meliodosis in an epidemic Asian area. Early suspicion may avert untowards fatal consequences and improved the quality of life.
A 59 years old Indonesian expatriate male who is a chain smoker farmer and housebuilder with no known medical illness presented at Emergency Department, Hospital Teluk Intan, Malaysia with chief complain of acute shortness of breath and severe frontal headache (pain score 7/10). The headache was throbbing in nature but not associated with nausea, vomiting, periorbital pain nor joint pain. In addition, He also had history of prolonged low grade fever and non productive cough for 5 days. There was no complain of chest pain, epigastric pain or limb weakness. There was no history of recent travelling to oversea or jungle trekking. He was also not living in dengue prone area and no recent dengue case or recalled any direct contact with the truberculous-infected persons.
In the emergency department, he was given BiPAP and Nebuliser. Salbutamol (5 mg) 2 hourly and was imediately instituted intravenous Augmentin (1.2 g) for a suspicion of acute exarcerbated chronic airway disease secondary to community acquired pneumonia complicated in sepsis. The differential diagnoses were pulmonary TB and dengue fever. Vital sign showed temperature of 38°C, blood pressure 110/70 mmHg, pulse rate tarcycardic 130 bpm, respiratory rate of 40 bpm with spO2 80%.
After day 2 of admission, the patient developed pleuritic chest pain, frequent cough, and bilateral leg swelling with further deterioration of, shortness. Physical examination suggestive of bibasal pleural effusion predominantly affecting the right lung. However there were signs of, body rashes, abdominal pain, hepatosplenomegaly or, cervical lymphadenopathy. Full blood count, renal profile, cardiac markers and coagulation profile showed no significant findings with normal ECG findings. His chest X-ray revealed multiloculated parapneumonic effusion of the both lung with higher meniscus at the right lung (Figure 1). Dengue serology done was negative.
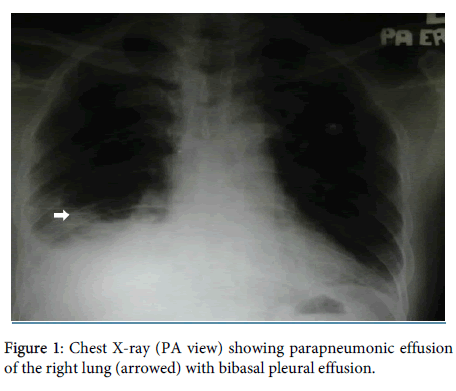
Figure 1: Chest X-ray (PA view) showing parapneumonic effusion of the right lung (arrowed) with bibasal pleural effusion.
Non-specific Blood cultures and sensitivity repeated and pleural fluid showed no pathogenic bacterial growth. Serum Acid Fast Bacilli, Tb PCR cytology and gram staining also were all normal. Intravenous Ceftazidime (Fortum) 2 g and 1 g tds were given with a combined Tablet Azythromycin (500 mg). A final diagnosis of meliodosis was made following a positive IGM-ELISA IGM titre blood serology for meliodoisis.
A shortness of breath was still not improving after pleural tapping, and second chest X-ray performed at day 5 of admission remains unchanged. He was given intravenous Hydrocortisone 200 mg stat and 100 mg PRN with Nebuliser Combivent at 4 hourly intervals. Fever was resolved at day 5 of illness followed by and resolution of all the, biochemical results. The patient was discharged well with eradication therapy after 2 weeks of hospitalisation. Oral Cotrimoxazole (500 mg) OD for 4 weeks was given and referred to primary clinic for regular follow up.
Study in Pahang, Malaysia showed 14.8% of the cases of meliodosis has no predisposing factor and the remaining percentage with underlying disease or predisposing factor [4-11]. This particular patient had several predisposing factors among which were cigarrete smoking and high exposure to the farming soil organism. A study also has noted that 93% of patients present with fever with median duration of 7 days to a maximum of 90 days [11] which substantiate the prodromal period of the disease manifestation in this particular report.
Melioidosis is a multisystem disease and the sign and symptom are nonspecific [11]. The wide range of clinical presentations include severe community-acquired pneumonia, septicaemia, central nervous system infection and less severe soft tissue infection [7]. This patient had pulmonary manifestation [9] without any other organ involvement and he only developed multifocal parapneumonic effusion which is classical on CXR. This is in line with the reported incidence of 1000 cases seen in Northeast Thailand, for which meliodosis (68%) with peculiar radiological abnormalities [9]. Unilateral pulmonary shadowing (56%) was more common with predominant involvement of the right lung. More than one lobe was affected in one out of five patients. Eventhough his clinical presentations were highly suggestive of community acquired pneumonia, Meliodosis is exeptionally a-not-to-be-miss diasgnosis in an epidemic Asian area with the mentioned prediosposisng factors. All the investigation findings were insignificant except for the IGM-ELISA titre and specific culture for psedomonas few days after hospitalisation. The use of laboratory discovery pathway such as serology can help reduce the risk of missing atypical B.pseudomallei isolates [5,7] as at times diagnosis is difficult given its resemblance with other bacteria species.The immediate institution of a personalised therapy of Ceftazidime (Fortum) [12] and T.Augmentin have ensured good prognosis in this patient. Review of a literature reveals most patients had successful treatment with a combination of Ceftazidime and Co-Trimazole in immediate therapy [12]. The patient was then continued with Oral Cotrimoxazole (500 mg) OD for 4 weeks for complete eradication and to prevent potential remission as total disease eradication of the organism is deemed difficult should the standard therapy is incompleted [10,13].
Melioidosis should not be forgotten and must be explicitly excluded especially in patient with low grade fever with atypical pneumonic changes on CXR with and the associated predisposing factors in an epidemic Asian area. Early suspicion and treatment institution are important to avert the untowards fatal consequences.