Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Case Report - (2016) Volume 5, Issue 3
We report the case of a 17 year old male patient, hospitalized for the evaluation of bleeding diarrhea with glairs. Colonoscopy and colonic biopsies allowed the diagnosis of ulcerative colitis (UC) in pancolitis. The patient put under corticosteroid and azathioprine. The evolution was marked by the disappearance of bleeding diarrhea. Faced with persistent iron deficiency anemia despite clinical remission, which worsened during the evolution and absence of geophagia or a capital deficiency, a gastroscopy was performed, the upper gastrointestinal endoscopy has not objectified visible macroscopic anomaly, however pathological study of duodenal biopsies showed partial villous atrophy with intraepithelial lymphocytoce. After the suspicion of a celiac disease, the assessment was completed by an immunological study that showed anti-gliadin antibodies and endomysial antibodies. The patient was put under gluten-free diet associated with the maintenance treatment of ulcerative colitis. On the occasion of this observation, we emphasize the rarity of this association and we the complex pathogenesis of celiac disease that could have similarities with that of ulcerative colitis.
Keywords: Association; Celiac disease; Ulcerative colitis
Celiac disease is an autoimmune enteropathy caused by the ingestion of gluten in genetically predisposed subjects. It is characterized by malabsorption due to total or subtotal villous atrophy of the proximal small intestine regressing after gluten free diet. The hemorrhagic ulcerative colitis, meanwhile, is a cryptogenic inflammatory bowel disease (IBD) affecting choice with the left colon, by relapses, interspersed with remissions. These two diseases affect favorite with young adults, though their association in the same patient has been rarely described. Some clinical cases and recently published series have suggested some relationship between the two disorders [1,2]. We report a new case of association between celiac disease and ulcerative colitis through which we discuss the etiopathogenic relationship between these two diseases.
Observation
This was a patient aged 17 year old with no personal history or significant pathological family, admitted to our training to record a chronic bleeding diarrhea with glairs amounted to 6 stools per day, along with a rectal syndrome and weight loss appeared six months earlier. Clinical examination revealed a patient emaciated, weighs 40 kg for 1.56 m, mucous cutaneous pallor biology find a hypochromic microcytic anemia (hemoglobin = 8.4 g/dl, MCV = 75 u3, MCHC = 28%), inflammatory syndrome (VS = 80 mm), and a carentiel syndrome. Liver function tests and blood electrolytes were normal. Parasitology of stools and stool cultures are negative. Colonoscopy has found a fragile mucosa erythematous weeping blood, with superficial ulceration and pseudopolyps, moving one piece from the anal verge to the caecum with a normal appearance last ileal loop (Figure 1). Colonic biopsies note an often ulcerated or peeled epithelium resting on a congestive edematous chorionic separated by a polymorphic inflammatory infiltrate, then the diagnosis of ulcerative colitis ulcerosa is placed and the patient is treated by parenteral corticosteroid for 5 days and then orally relay, 5-aminosalicylic acid enema and azathioprine for maintenance treatment. The evolution is marked by the disappearance of bleeding diarrhea and rectal syndrome but with persistence of anemia and impaired general condition. The patient was readmitted three months later; an upper endoscopy was then performed and revealed normal optically, and systematic gastric and duodenal biopsies are performed duodenal biopsies show partial villous atrophy and lymphoplasmacytic infiltrate and the increased number of intraepithelial lymphocytes (Figure 2). Immunologically there in the serum of gliadin IgA antibodies (1/1 600 identified by ELISA) and endomysial antibody (1/800, highlighted by the technique of immunofluorescence). The diagnosis of celiac disease is then retained and the patient is put under gluten-free diet the patient is reviewed regularly in consultation, gluten-free diet is properly followed. The evolution is marked by a resumption of weight (48 kg), a negativity gliadin and anti-endomysium associated decline in two years.
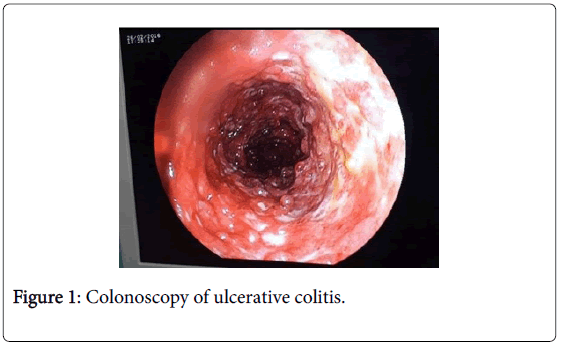
Figure 1: Colonoscopy of ulcerative colitis.
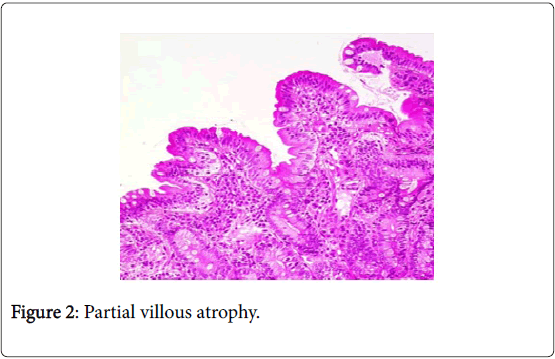
Figure 2: Partial villous atrophy.
Coeliac disease is an inflammatory disease, genetically determined in the small intestine. Its association with other autoimmune diseases such as type I diabetes and autoimmune thyroiditis is the clearly established [3]. However, its association with IBD is rare and the first case of celiac disease and Crohn's disease association was reported in 1967 [4]. Several recently published studies have reported an increase in the prevalence of IBD in patients with celiac disease [2,5]. In a recent Spanish series, this prevalence becomes eight times greater for people with celiac disease than in the general population [5]. The Increased risk of such an association also extends to first-degree relatives [5]. A Swedish study suggests that not only is there an association between IBD and celiac disease, but when they occur together, the risk of complications, sometimes fatal, increases [6]. This association occurs most often in the young adult male and poses a diagnostic problem. The diagnosis of celiac disease can be indeed difficult, especially in a patient already reached IBD. In fact, the two conditions often have common symptoms, such as diarrhea, weight loss and abdominal pain.
Endoscopic and histological aspects most characteristic of celiac disease may be observed in patients with IBD. Culliford et al. [7] have recently published three cases of duodenal Crohn's disease mimicking the aspect endoscopic of a celiac disease with villous atrophy in histology. This underlines the advantages of seeking the intraepithelial hyperlymphocytosis greater than 30% which is specific for celiac disease. The immunological balance should contribute to the differentiation between the two diseases. Anti-endomysial antibodies are specific to celiac disease and are not present in Crohn's disease or hemorrhagic ulcerative colitis [8]. However, anti transglutaminase can be found in IBD [8]. The anti-Saccharomyces cerevisiae antibodies present in 50-65% of cases of IBD can be observed during celiac disease [9]. Such findings suggests similarities between the two diseases and raise the possibility of similar etiopathogenic mechanisms involving immunological abnormalities. Etiopathogenic links between the two diseases are still poorly understood and several hypotheses have been advanced to explain such an association. The scarcity of similar cases reported in the literature may argue for a chance association [1]. The existence of familial forms of this association could evoke a particular genetic predisposition explains the concomitant occurrence of both diseases in the same individual [5].
The coexistence celiac disease and IBD is possible, although rare, evoking a particular genetic background and a similar pathogenesis involving immunological abnormalities. It should be suspected and sought by a comprehensive digestive balance in case of symptoms suggestive or therapeutic resistance to one of these two affections. A prospective and regular screening could reveal a greater incidence of this particular association and would assess the long term impact of each of these two diseases on the evolution of the other. The immunogenetic progress and analysis of similarities between these two diseases would further elucidate their pathophysiology.