Endocrinology & Metabolic Syndrome
Open Access
ISSN: 2161-1017
ISSN: 2161-1017
Research Article - (2018) Volume 7, Issue 4
Objective: Both glycine and cinnamon have been independently reported to favorably impact blood glucose. To our knowledge, no study has combined these two ingredients through oral supplementation in an attempt to modify the glycemic response to a glucose load. We determined the impact of acute ingestion of a novel glycine-cinnamon extract mixture on blood glucose, insulin, and related variables following an oral glucose challenge.
Methods: Ten men and women (25.4 ± 8.3 yrs) with elevated fasting blood glucose (101.2 ± 6.6 mg•dL-1) ingested a 25 gram glucose beverage with and without SugarClear™, a proprietary blend of glycine+cinnamon extract (as Cinnulin PF®), separated by approximately one week. Blood was collected before and at 20, 60, and 120 minutes post ingestion and analyzed for glucose, insulin, glucagon-like peptide-1 (GLP-1), glucagon, ATP, and brainderived neurotrophic factor (BDNF).
Results: Significant reductions in the area under the curve (AUC) were noted for both glucose (15% for total AUC and 52% for net incremental AUC) and insulin (7% for total AUC and 57% for net incremental AUC). The total AUC for GLP-1 was increased by 36%, while the AUC for ATP was increased by 20%. Glucagon was lower by 10% and BDNF higher by 5% with treatment but not in a statistically significant manner (p>0.05).
Conclusion: Acute ingestion of SugarClear™, a proprietary blend of glycine and cinnamon extract, promotes a positive impact on blood glucose and insulin following an oral glucose load. The mixture also leads to an increase in both the plasma GLP-1 and ATP. These alterations may have favourable metabolic implications in those with elevated blood glucose. Future work is needed to determine the effect of chronic ingestion of SugarClear™ on glucose regulation and related variables.
Keywords: Glycine; Cinnamon; Blood glucose; Insulin; ATP; Prediabetes; Metabolic syndrome
Both glycine and cinnamon have been reported to have a favourable impact on blood glucose, which may be beneficial in improving metabolic health, in particular for those with slightly elevated fasting blood glucose (100-125 mg•dL-1) and considered to be pre-diabetic [1,2]. It is estimated that approximately 84 million adults living within the United States have pre-diabetes, many of whom can benefit from nutritional approaches aimed at reducing fasting and post-prandial blood glucose [3].
Glycine is an amino acid found in most protein-rich foods and has a number of physiological functions, including enhancing antioxidative capacity and improving immunity [4]. As a dietary supplement, glycine has received attention recently as a potential aid in regulating blood glucose. Iverson and colleagues reported a significant reduction in the glucose area under the curve (AUC) when glycine was added to a 25 gram glucose load ingested by nine subjects and compared to a placebo [1].
Cinnamon is a spice that is widely used in cooking but also has been reported to provide medicinal value, including a reduction in both blood glucose and blood pressure [5,6]. In vitro studies have shown that isolated compounds from cinnamon improve insulindependent glucose metabolism [7]. A human study with a cinnamon extract known as Cinnulin PF® has noted improved fasting blood glucose, among other benefits related to metabolic syndrome [8-10].
When collectively considering the evidence, we sought to determine the impact of a glycine+cinnamon extract mixture on blood glucose, insulin, and related variables in response to an oral glucose challenge. Specifically, glucose, insulin, glucagon, and glucagon-like peptide-1 (GPL-1) are important in controlling blood glucose, while ATP is of great important with regards to providing energy for working cells. We hypothesized that the glycine+cinnamon extract mixture would result in a lowering in the glucose and insulin AUC in response to glucose ingestion.
Subjects
A total of 10 men and women participated in this study. While this sample size is relatively small, it is quite common in research studies involving a cross-over design and of similar scope as the present design. In order to enroll all subjects, a total of 63 individuals were screened and only 10 met all inclusion criteria. Subjects needed to have/be: a non-smoker; without a diagnosed history of diabetes, cardiovascular disease, or neurological disease; no prior history of difficulty with venipuncture; a fasting blood glucose value between 95 and 125 mg•dL-1; a body index ≥ 28 kg•m-2 (in order to include those at the upper limit of overweight status or obesity status); physically active (two or more days per week of structured physical activity for a minimum of 30 minutes each day); not using cinnamon-containing supplements and not allergic to cinnamon; and if female, not pregnant.
Prior to participation, each subject was informed of all procedures, potential risks, and benefits associated with the study through verbal and/or written format. All procedures were approved by the University of Memphis Institutional Review Board for Human Subjects Research (#PRO-FY2018-58).
Initial laboratory visit: screening visit
During the initial visit to the laboratory, individuals completed the informed consent form, as well as health history, medication and dietary supplement usage, and physical activity questionnaires. For physical activity, subjects noted the frequency and duration of activities, involving aerobic (e.g., jogging, cycling) and anaerobic work (e.g., weight training), as well as sporting activities. This helps us to understand how much overall physical activity and exercise a person may be engaged in. A blood sample of approximately 20 μL (a single drop obtained via finger prick) was taken and analysed for blood glucose level using a glucometer (One Touch Ultra). Individuals’ heart rate and blood pressure, height, weight, waist, and hip circumference were measured using standard procedures. Women completed a urine pregnancy test to confirm that they were not pregnant. Upon completion of the screening, eligible individuals were scheduled for their initial testing visit.
Conditions
Subjects were randomly assigned to ingest either a 25 gram (~100 calorie) carbohydrate beverage (dextrose) with no additional ingredients (placebo condition) or the same 25 gram beverage with the addition of glycine and cinnamon extract. The glycine-cinnamon extract mixture was provided by IN-Ingredients as SugarClear™, a proprietary blend of glycine and the cinnamon extract, Cinnulin PF®, which is water soluble, 20:1 extract containing doubly-linked polyphenol type-A polymers. The two beverages were consumed on two separate days, with approximately one week between visits. This 25 gram, 100 calorie beverage served as our oral glucose tolerance test (OGTT) and provided the same calorie load as used by Iverson and coworkers in a similar design involving glycine [1]. One week prior to this, subjects consumed the same placebo beverage without any additional ingredients in order to serve as a familiarization/baseline trial. Therefore, subjects consumed the beverage a total of three times over a three-week period. The beverages were very sweet and similar in test. Due to the sweet flavour of the beverage, the addition of glycine and cinnamon extract did not significantly alter the flavour profile.
Laboratory test visits
Subjects reported to the lab in the morning hours following an overnight fast (10+ hours) on a total of three occasions over a 3 weeks period in a randomized, blinded, cross-over study. Subjects were instructed to obtain at least 7 hours of sleep the night prior, as lack of sleep is known to negatively impact glucose tolerance [11]. Upon arrival to the lab, subjects rested quietly for 20 minutes and then had a blood sample taken (approximately 10mL). Their blood pressure was then measured and they completed a standard questionnaire related to how they felt. Subjects then received their assigned beverage (approximately 12 ounces) and were instructed to consume all of it within 5 minutes. Additional blood samples were taken at 20, 60, and 120 minutes post ingestion. Blood pressure and the questionnaire responses were recorded at these times also. No other food or calories containing beverages were allowed during the two-hour collection period. At the end of the two-hour data collection period, subjects were allowed to leave the lab.
Blood collection and analyses
The collected samples were processed and stored in multiple aliquots at -70 degrees Celsius. Although multiple outcome variables could have been included in this design, we selected variables that were most likely to be impacted by the ingredients being tested. Plasma glucose was determined using a glucose analyser (OneTouch glucose meter, LifeScan Europe, Switzerland). Plasma insulin, brain-derived neurotrophic factor (BDNF) and glucagon concentrations were measured using commercially available enzyme-linked immunosorbent assay (ELISA) kits: human Insulin ELISA Kit (Abcam, Cambridge, MA), human BDNF PicoKine ELISA kit (Boster, BIO, Pleasanton, CA), and the Glucagon Quantikine ELISA Kit (R&D Systems, Minneapolis, MN), according to the manufacturers’ instructions. Total GLP-1 was measured on a microplate reader (Spectra Max, Molecular Devices, San Jose, CA) using a multi-species total GLP-1 ELISA kit (EZGLP1T-36K; Millipore). For analysis of plasma adenosine triphospharte (ATP), one hundred μl of blood was transferred to low protein binding tubes, immediately after collection. An equal volume of ATP stabilizing solution was added to each tube. Tubes were gently mixed by inversion and centrifuged at 13,000 g for 3 min to pellet cells. The supernatant was transferred to a clean tube and spun again at 13,000 g for 3 min. The supernatant was then stored at -70°C prior to ATP analysis. Total plasma ATP concentration was determined using ATP Detection Assay Kit (Cayman Chemical, Ann Arbor, Michigan). The area under the curve (AUC) for glucose, insulin, BDNF, glucagon, GLP-1, and ATP was calculated with the use of the trapezoidal method for total AUC [12]. Incremental AUC was also calculated for both glucose and insulin.
Activity and dietary intake
Subjects were instructed to maintain their usual activity patterns throughout the study period but refrain from strenuous physical activity during the 48 hours prior to each test day visit. Subjects were also instructed to maintain their usual dietary intake throughout the study period and record all food and drink consumed during the twoday period prior to each test day. Diet records were analysed for macronutrient and micronutrient intake using dietary software (Food Processor Pro, Esha Research, and Salem, OR).
Data analysis
Data are expressed as mean ± SD. The significance of differences was evaluated using Student’s t-test in Microsoft Excel (Microsoft, Richmond, WA). Statistical significance was determined at p<0.05.
All 10 subjects successfully completed the study. Descriptive characteristics are presented in Table 1. Dietary data were not different during the two days prior to each test day. Data are presented in Table 2.
| Variable | Men |
|---|---|
| Age (years) | 25.4 ± 8.3 |
| Height (cm) | 169.7 ± 12.4 |
| Body Weight (kg) | 91.7 ± 17.9 |
| Body Mass Index (kg∙m-2) | 31.6 ± 2.8 |
| Waist Circumference (cm) | 97.8 ± 10.5 |
| Hip Circumference (cm) | 111 ± 8.0 |
| Waist:Hip | 0.88 ± 0.04 |
| Heart Rate (bpm) | 67.3 ± 10.8 |
| Systolic Blood Pressure (mmHg) | 122.5 ± 14.2 |
| Diastolic Blood Pressure (mmHg) | 76.2 ± 5.7 |
| Fasting Blood Glucose (mg∙dL-1) | 101.2 ± 6.6 |
Table 1: Characteristics of men and women.
| Variable | Placebo I (Familiarization) | SugarClear™ | Placebo II |
|---|---|---|---|
| Kilocalories | 1972 ± 675 | 1870 ± 449 | 1929 ± 422 |
| Protein (g) | 96 ± 53 | 93 ± 68 | 93 ± 48 |
| Carbohydrate (g) | 224 ± 65 | 188 ± 61 | 216 ± 77 |
| Fiber (g) | 17 ± 5 | 17 ± 6 | 15 ± 4 |
| Sugar (g) | 91 ± 52 | 49 ± 35 | 67 ± 42 |
| Fat (g) | 78 ± 39 | 82 ± 36 | 72 ± 25 |
| Vitamin C (mg) | 59 ± 52 | 47 ± 35 | 60 ± 53 |
| Vitamin E (mg) | 2 ± 2 | 4 ± 4 | 2 ± 2 |
| Vitamin A (RE) | 458 ± 279 | 339 ± 323 | 254 ± 150 |
Values are mean ± SD
No difference of statistical significance noted (p>0.05)
Table 2: Dietary data of subjects during the 48 hours prior to each test day.
Related to the OGTT, compared to the placebo, plasma glucose levels at 20 minutes and 60 minutes were lower in the SugarClear™ group (p<0.05; Figure 1A). Moreover, the AUC was lower for the SugarClear™ group (Table 3). When considering the total AUC, glucose in the SugarClear™ group was noted to be approximately 15% lower as compared to placebo (p=0.02), while the net incremental glucose AUC was approximately 52% lower than placebo (p=0.05).
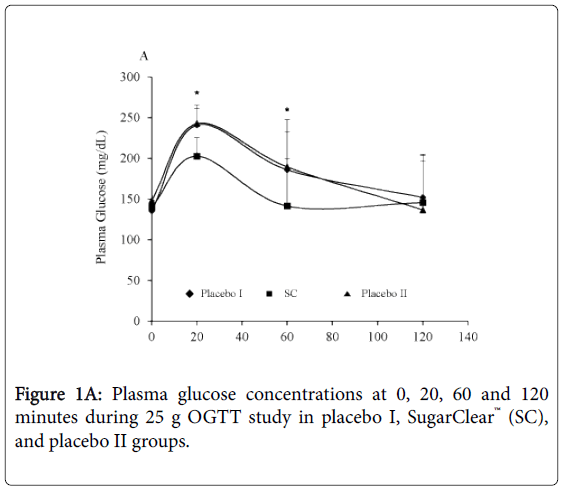
Figure 1A: Plasma glucose concentrations at 0, 20, 60 and 120 minutes during 25 g OGTT study in placebo I, SugarClear™ (SC), and placebo II groups.
| Placebo I (Familiarization) |
SugarClear™ | Placebo II | |
|---|---|---|---|
| Glucose AUC (mg∙dL-1∙120min-1) | 22438 ± 3620a | 18918 ± 3190b | 22352 ± 4036a |
| Insulin AUC (mU∙L-1∙120min-1) | 1441 ± 250a | 1269 ± 177b | 1371 ± 202ab |
| GLP-1 AUC (pg∙mL-1∙120min-1) | 7744 ± 3387a | 9987 ± 4462b | 7342 ± 2709a |
| ATP AUC (mMol∙L-1∙120min-1) | 6444 ± 2839a | 7492 ± 3138b | 6240 ± 2750a |
| Glucagon AUC (pg∙mL-1∙120min-1) | 9114 ± 2528a | 7398 ± 1937b | 8275 ± 2569ab |
| BDNF AUC (pg∙mL-1∙120min-1) | 19020 ± 3338a | 20002 ± 2430a | 19043 ± 2464a |
Data are presented as mean±SD
Values within a row without a common letter superscript differ from one another (p<0.05)
Table 3: Total AUC of plasma glucose, insulin, GLP-1, ATP, glucagon, and BDNF following an oral glucose tolerance test.
Plasma insulin levels at 60 minutes were lower in the SugarClear™ group compared to placebo (p<0.05; Figure 1B). As with glucose, the AUC for insulin was lower for the SugarClear™ group as compared to placebo (Table 3). When considering the total AUC, insulin in the SugarClear™ group was noted to be approximately 7% lower as compared to placebo (p=0.11), while the net incremental insulin AUC was approximately 57% lower than placebo (p=0.03).
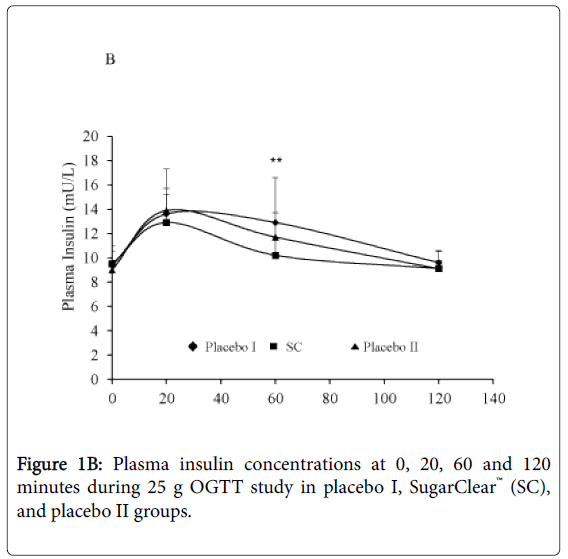
Figure 1B: Plasma insulin concentrations at 0, 20, 60 and 120 minutes during 25 g OGTT study in placebo I, SugarClear™ (SC), and placebo II groups.
As shown Figure 2A, total plasma GLP-1 levels in the SugarClear™ group at 60 minutes are higher compared to placebo (p<0.05). At 120 minutes, a trend was noted, with increased plasma GLP-1 levels in the SugarClear™ group compared to placebo (p=0.06). The AUC of GLP-1 in the SugarClear™ group was higher than placebo by approximately 36% (p=0.05; Table 3).
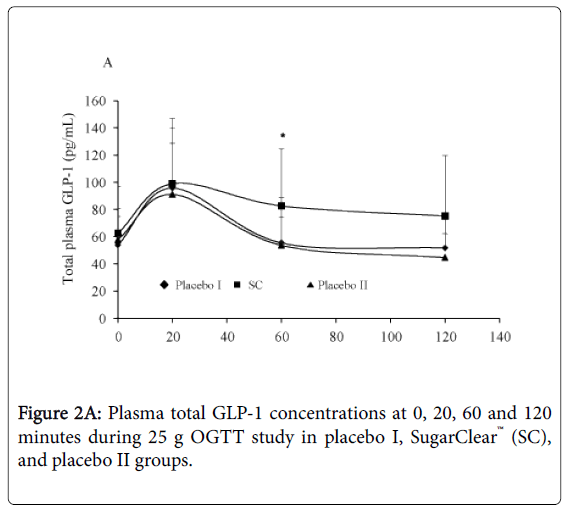
Figure 2A: Plasma total GLP-1 concentrations at 0, 20, 60 and 120 minutes during 25 g OGTT study in placebo I, SugarClear™ (SC), and placebo II groups.
As shown in Figure 2B, there was a strong trend of increased plasma ATP levels in the SugarClear™ group at 20 minutes, 60 minutes and 120 minutes compared to placebo. The AUC was increased by approximately 20% in the SugarClear™ group (p=0.02; Table 3). The sample for subject 8 at 60 minutes post-ingestion of the SugarClear™ condition was not analyzed for ATP due to an insufficient volume to process for ATP analysis and obtain plasma.
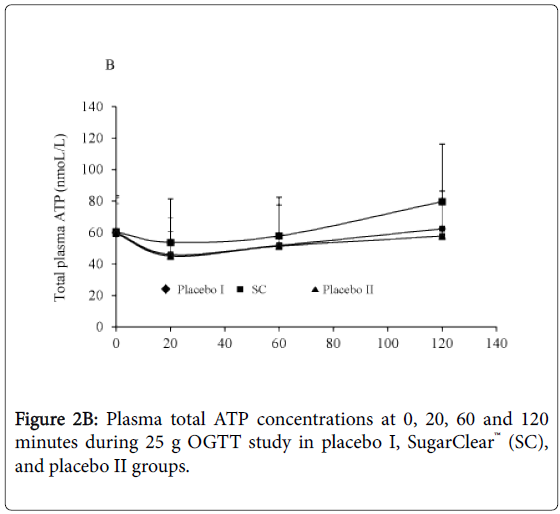
Figure 2B: Plasma total ATP concentrations at 0, 20, 60 and 120 minutes during 25 g OGTT study in placebo I, SugarClear™ (SC), and placebo II groups.
As shown in Figure 3A, plasma glucagon levels were not different between the SugarClear™ group and placebo (p>0.05), nor were there statistically significant differences in the AUC (p=0.22; Table 3), despite an approximate 10% decrease in glucagon for the SugarClear™ group compared to placebo.
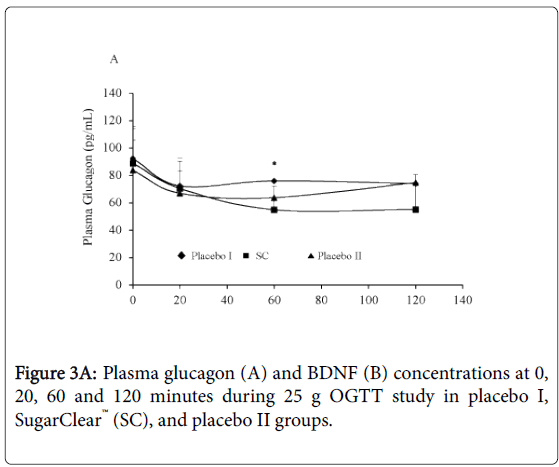
Figure 3A: Plasma glucagon (A) and BDNF (B) concentrations at 0, 20, 60 and 120 minutes during 25 g OGTT study in placebo I, SugarClear™ (SC), and placebo II groups.
As shown in Figure 3B, a trend was noted for increased plasma BDNF levels in the SugarClear™ group at 120 minutes compared to placebo (p=0.08). No differences of significance were noted for AUC for BDNF (p>0.05; Table 3).
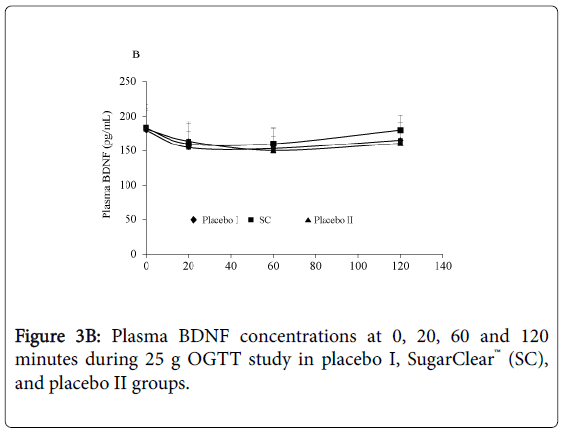
Figure 3B: Plasma BDNF concentrations at 0, 20, 60 and 120 minutes during 25 g OGTT study in placebo I, SugarClear™ (SC), and placebo II groups.
We also observed that there were no changes in heart rate or blood pressure between conditions or across time. Finally, subjective mood was not impacted by condition or time (data not shown).
The objective of this study was to determine if SugarClear™ increases glucose disposal, in addition to having other positive and related metabolic effects. These effects may help to support dietary manipulations aimed at minimizing rises in blood glucose, perhaps in accordance with a low carbohydrate diet. Our findings indicate that the combination of glycine and the cinnamon extract can favourably impact blood glucose and insulin following glucose ingestion, while also having a positive impact on circulating GLP-1 and ATP levels.
Maintaining a low to moderate blood glucose level is important to overall health-at rest, following acute feeding, and during acute exercise sessions [13-15]. It is also beneficial to individuals who have impaired glucose tolerance (IGT) and who present with elevated blood glucose levels, generally >100 mg•dL-1, but who are not yet classified as diabetic. IGT has been associated with blood vessel damage, liver problems, pancreas islet cell and beta cell dysfunction, and nerve damage [16-18]. Our data support the use of the glycine-cinnamon extract mixture to maintain lower blood glucose levels in response to the ingestion of simple sugar.
The mixture, SugarClear™, is made up of a proprietary blend of glycine and the cinnamon extract known as CinnulinPF®. Glycine is an amino acid, simple in structure (NH2CH2COOH) and made within the liver with single hydrogen that makes up the side chain. Large amounts of glycine are found in human muscle, connective tissue, and skin. As a supplement, glycine has a protective effect on muscle mass and function, and assists in cellular homeostasis [19]. Glycine assists in converting glucose to energy, which appears to aid in maintaining blood glucose levels.
Glycine has been shown within cells to stimulate an increase in GLP-1 secretion in a GLUTag cell line from intestinal L-cells [20]. These cells are specialized for GLP-1 production within intestinal mucosal tissue. Glycine has been used previously with success in a small sample of nine subjects [21]. Subjects ingested 1 mmol glycine/kg lean body mass, 25 grams glucose, 1 mmol glycine/kg lean body mass plus 25 g glucose, or water only, provided randomly. Plasma glucose, insulin, glucagon, and glycine levels were measured. Those ingesting glycine experienced a rise in plasma glycine and glucagon, with a slight rise in insulin. The consumption of glycine and glucose caused the plasma glucose AUC to diminish by greater than 50% compared to consuming glucose by itself. Our data extend these findings by using a smaller dosage of glycine coupled with cinnamon, while observing similar effects on blood glucose lowering. In another study involving 74 subjects with type 2 diabetes, subjects were administered 5 grams of glycine and exhibited significantly lower HbA1C levels after 3 months compared to those assigned to a placebo [22]. These prior studies support the use of glycine as an agent to assist in the regulation of blood glucose-a finding that was observed in the present study using a single dose of glycine in combination with a cinnamon extract.
Cinnulin PF®, a 20:1 water soluble cinnamon extract, has been shown to improve aspects of blood glucose control in multiple studies. Ziegenfuss and colleagues assigned 22 pre-diabetic subjects to either Cinnulin PF® or placebo for 12 weeks [10]. The Cinnulin PF® group experienced reductions in fasting blood glucose, lower systolic blood pressure, and increased lean muscle mass compared to the placebo group. In another study, 22 subjects with impaired fasting blood glucose were noted as having improved blood glucose, as well as improvement in plasma malondialdehyde (MDA), a measure of lipid peroxidation, following Cinnulin PF® supplementation [8]. The finding related to MDA is important, as it has been shown that oxidative stress is linked to hyperglycemia, and chronic oxidative stress can adversely alter various signaling pathways [23]. Cinnulin PF® was administered in two other human studies with women with Polycystic Ovary Syndrome (PCOS). Treatment proved beneficial in both studies, with a noted significant reduction in insulin resistance [9] and improved menstrual cyclicity [24]. In one animal study of Cinnulin PF®, the treatment was added to a high fructose diet in rats and was noted to improve glucose, insulin, and other related biomarkers [25]. Our data extend the findings for cinnamon in relation to blood glucose regulation, while highlighting the additive effect of glycine.
The present study demonstrated that the SugarClear™ treatment had a favourable impact on blood glucose, as shown in Figure 1 and Table 3. This was in response to an acute ingestion of the supplement in combination with a 25 gram glucose load. These findings confirm the prior effects noted for both glycine and the cinnamon extract, as discussed above. Of most interest is the approximate 15% reduction in glucose total AUC with treatment and an approximate 52% decrease for net incremental AUC. AUC is an important representation of glucose levels over a period of time, as opposed to a single measurement, and is helpful when assessing postprandial hyperglycemia [26]. Related to the glucose effects, the treatment group had a small but meaningful impact on blood insulin, with an approximately 7-8% reduction in insulin total AUC noted with SugarClear™ and an approximate 57% decrease for net incremental AUC. Lower insulin levels in response to the SugarClear™ treatment may be due to a heightened insulin sensitivity, which may reduce the need for additional insulin to be secreted. It is possible that chronic ingestion of the supplement may have a more robust effect-a hypothesis that requires further testing in a subsequent study.
Aside from glucose and insulin, we included additional measures in the present study that we believe are related and have merit in the context of metabolic health. Glucagon-like peptide-1 (GLP-1) is a neuropeptide hormone and also an incretin that, when increased, has a positive effect on blood glucose [27]. We observed a significant (36%) increase in GLP-1 AUC with the SugarClear™ treatment compared to placebo. GLP-1 promotes insulin secretion to help provide blood glucose balance, while reducing glucagon levels [28]. In addition, GLP-1 delays gastric emptying, which may lead to increased satiety and reduced calorie intake [29]. In individuals with poorly controlled and elevated blood glucose, increased GLP-1 may prove helpful to weight management.
From a mechanistic standpoint, the enzyme dipeptidyl peptidase IV (DPP-IV) converts GLP-1(7-36) into the inactive GLP-1(9-36). Adenosine deaminase (ADA) is an essential protein involved in the control of both intracellular and extracellular adenosine activity in the body [30]. It has been suggested that inhibiting DPP-IV and ADA would be helpful in treating diabetes mellitus [31]. Cinnamon has been shown to be effective in inhibiting DPP-IV and ADA and suggested to be beneficial to individuals with blood glucose problems [31]. Cinnamon has also been shown to significantly increase the GLP-1 response when added to rice pudding [32]. Our findings of increased GLP-1 AUC in the SugarClear™ group correlates with these findings.
Adenosine-50-triphosphate (ATP) is the body’s main intracellular energy source and acts as a signalling molecule assisting cells and tissues in communication [33,34]. ATP provides the foundation for the adenosine in DNA and RNA. It also has specialized functions in extracellular spaces facilitated through purinergic (P2Y and P2X) membrane receptors found in various cells [35]. We observed a significant (20%) increase in the ATP AUC with the SugarClear™ treatment. The overall impact of this finding is presently unknown but merits further investigation, ideally involving a functional assessment (e.g., physical exercise) coupled with the blood measurement of ATP.
Finally, we measured glucagon and BDNF, both of which experienced only an insignificant change with SugarClear™ treatment (10% decrease and 5% increase, respectively). While glucagon is wellknown to be associated with glucose, BDNF is a protein and a neurotransmitter modulator involved in neuronal plasticity, important for learning and memory [36]. BDNF is involved in the metabolism of glucose and energy and diminishes Beta cell fatigue [36]. It is believed that BDNF plays a role in protecting against the advancement of type 2 diabetes [37]. Further research with a larger sample size is needed to more fully elucidate the impact of the SugarClear™ treatment on BDNF and functional outcomes associated with this measure.
We noted that acute ingestion of SugarClear™, a proprietary blend of glycine and cinnamon extract, promotes a positive impact on blood glucose, insulin, GLP-1, and ATP levels following acute, oral ingestion of glucose in those with elevated blood glucose. These findings may have implications for those with elevated blood glucose, seeking methods of better glucose control. Moreover, those who desire enhanced glucose disposal following carbohydrate feedings (e.g., athletes and fitness enthusiasts) may benefit from the glycinecinnamon extract mixture. Future intervention studies are needed to determine the impact of chronic ingestion of SugarClear™ on metabolic control and related functional outcomes, while possibly separating the impact of both glycine and cinnamon extract, while using a larger sample size.
Funding for this work was provided in part by IN-Ingredients and The University of Memphis.
RJB was responsible for the study design, study oversight, and manuscript preparation. MB was responsible for subject recruitment and screening, data collection, and database management. JQT was responsible for assistance with manuscript preparation. BQ was responsible for the biochemical work and statistical analyses. All authors read and approved of the final manuscript.
JQT and BQ are scientists affiliated with IN-Ingredients, who assisted in funding this work. Neither RJB nor MB have affiliations with IN-Ingredients and declare no competing interests.