Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Review Article - (2016) Volume 5, Issue 2
The BTA guidelines for the management of thyroid nodules and cancer have been widely adopted in the UK. We have been applying them in our routine clinical practice for over a year now and we would like to share some of our experiences. Overall, we believe that they are having a positive impact on the management of these conditions, for example the U-classification of thyroid nodules allows for a more structured way of classifying nodules and communicating information. Nevertheless, we would like to highlight some areas of concern and which may form the focus of future modifications of the guidelines and/or research on this topic.
<Keywords: Thyroid nodules; Thyroid cancer; Ultrasound; Vascularity; Multi-nodular goiter; Elastography
We would like to take this opportunity to critique on the general use of the BTA guidelines for the management of thyroid nodules and cancer [1]. These guidelines have overall been welcomed and widely adopted by the communities of endocrinologists, radiologists, surgeons and oncologists in the UK and, to some extent, elsewhere in Europe. For example, the U-classification (Table 1) encourages the sonographer to translate his findings into a specific degree of concern and allows for a common language among health care professionals to communicate ultrasound findings. However, there are some areas where the guidelines may be controversial and others that have limited applicability in day-to-day practice.
| U-score | Nodule characteristics on USS | 1st FNAneeded | 2nd FNA needed |
|---|---|---|---|
| 1 | Normal thyroid | No | No |
| 2 | Benign e.g. isoechoic or mildly hyperchoic, halo present, spongiform, fully cystic, egg-shell calcification, peripheral vascularity and colloid seen |
No† | No |
| 3 | Indeterminate e.g. mildly hypoechoic, possible echogenic foci, solid and markedly hyperchoic (follicular lesion) and mixed vascularity |
Yes | Yes |
| 4 | Suspicious for malignancy e.g. solid, hypoechoic or very hypoechoic, disrupted peripheral calcification and lobulated lesion |
Yes | Yes |
| 5 | Likely malignant e.g. solid hypoechoic with microcalcifications (PTC) and macrocalcifications (MTC), lobulated, abnormal lymph nodes, internal vascularity and taller-than-wide shape |
Yes | Yes |
Table 1: U-score classifications on thyroid ultrasound scan (USS) and recommended actions depending on the actual score; adapted from BTA guidelines [1]. FNA: Fine-needle Aspiration; PTC: Papillary Thyroid Carcinoma; MTC: Medullary Thyroid Carcinoma. †FNA can be performed if the patient is deemed to belong to a high risk group i.e. if there is a family history of thyroid cancer or previous exposure to ionizing radiation.
Vascularity
Mixed and internal vascularity are classed as U3 and U5 respectively, according to the BTA guidelines. Given that in real practice some degree of internal vascularity is common and its presence is considered a somewhat ‘softer’ sonographic feature of malignancy [2-4], then if these criteria are strictly adhered to, that would likely lead to an increased amount of nodules labelled as ‘indeterminate’ (U3) and ‘likely malignant’ (U5) with the inherent risk of more FNAs performed, more anxiety and potentially more unnecessary surgeries carried out.
Elastography
Elastography is not currently incorporated into the U-classification, albeit the guideline authors do acknowledge its potential to be integrated into the aforementioned classification. We believe that it can be used as a supplementary tool especially in indeterminate cases (U3 or U2/U3) and has the potential to flip the balance in the direction of fine-needle aspiration (FNA) or no FNA, depending on whether the nodule tissue is elastic or stiff, respectively [5,6]. With the increased availability of sonographic devices that have elastography as an inbuilt function, it is likely that this tool will become more widely utilised. However, its full potential is still unclear especially given that many trials have reported different results and one need to be aware of some caveats with it such as its inability to be used for cystic or significantly calcified nodules [5].
Nodules on computed tomography (CT) and magnetic resonance imaging (MRI)
The current recommendation by the BTA is to clinically assess and examine nodules that are incidentally identified on CT or MRI scans; if no abnormalities are found on clinical evaluation, the recommendation is that there is no need for any ‘further assessment / investigations’. A provision on the guidelines includes an exception for those nodules that exhibit tracheal invasion, extra-capsular invasion or associated abnormal lymph nodes (all of which are rare) and also for patients belonging to a high-risk group. However, the clinical examination of nodules is less sensitive than ultrasound and this is especially true for sub-centimetre nodules [7]. Bearing in mind that palpation is more susceptible to inter-observer variability and given a lesser reliance on nodule size nowadays (versus other morphologic appearances on ultrasound); the justification for such an approach is weak. Moreover, it is unclear who should perform the physical examination. For example, is the general practitioner or physician that requested the initial scan, responsible for examining the patient and for deciding whether to proceed with an USS examination or not? If the patient is referred to an endocrinologist as is often the case, most endocrinologists would feel uncomfortable with dismissing such a lesion without a sonographic assessment, especially in the current litigation environment and given the easy access to high-resolution thyroid USS.
Multi-nodular goitre (MNG)
It is possible that the guidelines may be too aggressive when it comes to the management of MNG. In our experience U3 features such as possible hypoechogenicity, equivocal echogenic foci and cystic change are very common among MNG (Figure 1). The question arises whether all nodules that display such features (which could be multiple in a single patient) and in the absence of more concerning signs (marked hypoechogenicity, microcalcifications, irregular margins and/or taller-than-wide) should be targeted with FNA. Furthermore, macrocalcifications are common in MNG but it is not clear in the BTA guidance whether such nodules should be managed more aggressively.
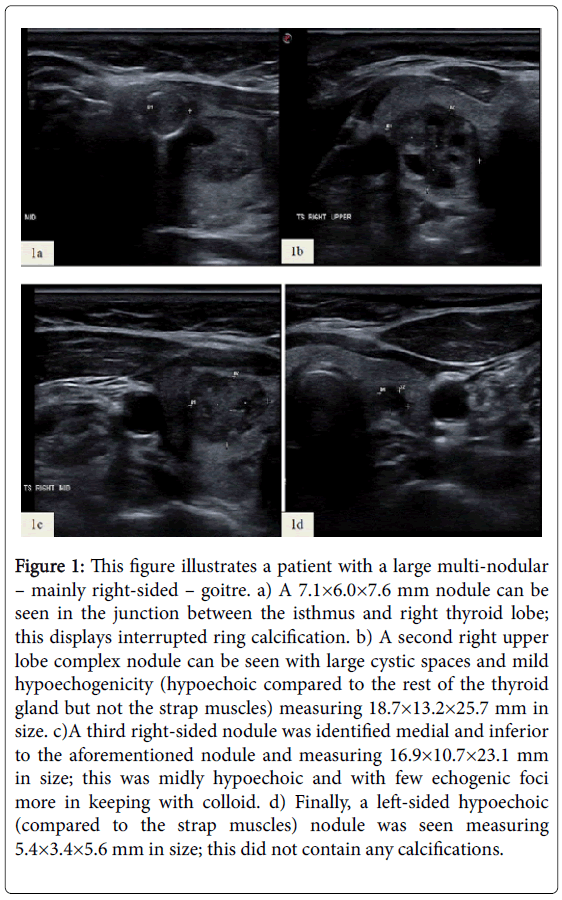
Figure 1: This figure illustrates a patient with a large multi-nodular – mainly right-sided – goitre. a) A 7.1×6.0×7.6 mm nodule can be seen in the junction between the isthmus and right thyroid lobe; this displays interrupted ring calcification. b) A second right upper lobe complex nodule can be seen with large cystic spaces and mild hypoechogenicity (hypoechoic compared to the rest of the thyroid gland but not the strap muscles) measuring 18.7×13.2×25.7 mm in size. c)A third right-sided nodule was identified medial and inferior to the aforementioned nodule and measuring 16.9×10.7×23.1 mm in size; this was midly hypoechoic and with few echogenic foci more in keeping with colloid. d) Finally, a left-sided hypoechoic (compared to the strap muscles) nodule was seen measuring 5.4×3.4×5.6 mm in size; this did not contain any calcifications.
All nodules had predominant peripheral vascularity. Thyroid FNA was undertaken in all these nodules successfully, but the procedure was prolonged given the need for 3 passes × 4 nodules and also the fact that the patient suffered some minor bleeding which was well controlled with pressure with a tissue. Not suprising the patient found the whole procedure somewhat traumatic. The results indicated a Thy 2 cytology from all nodules. Given that none of these nodules would fit in with a U2 classification, if the guidelines are to be strictly adhered to then it means that they should all be re-sampled with FNA which is not a trivial undertaking. This is not an uncommon conundrum in daily clinical practice.
Ultrasound criteria in dynamic risk stratification at 9-12 months after total thyroidectomy and radioiodine ablation state that patients with stable sub-centimetre lymph nodes are stratified as ‘indeterminate responders’. Given that small and benign lymph nodes are common, then if this criterion is strictly adhered to, that could lead to a lot of patients being labelled as ‘indeterminate responders’ with all the anxiety, additional investigations, follow-up and potentially extra treatments that come along with such a label. However, a different approach would be to simply classify any identified lymph nodes as benign or suspicious for malignancy based on the usual morphologic, size and Doppler criteria. The latter should be targeted with FNA even if sub-centimetre in size.
The authors declare that no competing financial interests exist.