Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Case Report - (2016) Volume 5, Issue 2
Esophageal epiphrenic diverticulum is not common clinical presentation. They result from various pathologies, usually due to the motility disorder that leads to the formation of the pouch through the weakened esophageal wall. Most of such large lesions usually associated with severe aggravating symptoms. Here we present a case of large epiphrenic diverticula with misleading nonspecific features of gastroesophageal reflux disease, where spontaneous recovery of symptoms was achieved with conservative treatment.
Keywords: Esophageal diverticula; Epiphrenic diverticula; Lower esophageal diverticula; Gastroesophageal reflux disease
ED: Esophageal diverticula; EED: Epiphrenic esophageal diverticula; ECG: Electrocardiography; ETT: Exercise tolerance test; GIT: Gastrointestinal tract; HP: Helicobacter pylori; MD: Middle third diverticula; VATS: Video-assisted thoracoscopic surgery; ZD: Zenker diverticula
Esophageal epiphrenic diverticula particularly a large one is a rare clinical presentation. They usually result due to motility disorders that cause spontaneous pressure over the weakened esophageal wall. Presenting symptoms of Epiphrenic esophageal diverticula depends on the underlying disease process and they mostly present with alarming symptoms.
The patient was a 65 years old Chinese man presented with recurrent heaviness and pain in the central chest and in the upper abdomen, which was exacerbated in last 6 months. The pain was moderate in nature, associated with heartburn and occasional food regurgitation. He was hypertensive, non-diabetic with a normal bowel movement. The patient had a habit of alcohol intake but no smoking. His ECG, ETT, echocardiography, and chest X-ray was normal. So, cardiac and pulmonary causes were excluded. On examination, his abdomen was found soft but moderate tenderness was detected in the epigastrium and the hypochondriac regions. Bowel sound was normal. Our patient had a previously treated history of Helicobacter pylori (HP) related gastritis few years back. His laboratory tests including blood routine, biochemistry, C14 Urea breath test for HP and abdominal ultrasound were insignificant. However, the esophagogastroduodenoscopy revealed features of chronic gastritis and large diverticula of about 5.5 × 3.5 cm with comparatively narrow opening and 6-7 cm depth in the lower third of the oesophagus along the left margin just above the lower esophageal sphincter. A small amount of residual food was observed in it. No ulceration or any other pathology was detected in the diverticula. His symptoms were clinically diagnosed as related to gastroesophageal reflux disease and gastritis so conservative treatment with diet modification, oral Rabiprazole and mosapride were advised. 10 days post treatment follow up with a plan for manometry was scheduled, if the symptoms did not respond to the prescribed treatment. Following treatment the patient’s condition improved and symptoms resolved spontaneously.
Esophageal diverticula (ED) are a rare presentation compare to the other of the gastrointestinal tract (GIT), around 1% of all GI barium radiograph. They are particularly prevalent in adult age group and can occur in all the three section of oesophagus. Diverticula in the upper, middle (MD) and lower third of the oesophagus referred as pharyngeal like Zenker diverticula (ZD), parabronchial and epiphrenic esophageal diverticula (EED) [1].
According to Pathophysiology they can be classified into pulsion and traction diverticulum. Traction diverticula occur because of chest infection leading to adhesion and fibrous change or scar formation that pull the section of the esophageal wall and form an outward bulging. In past days, they were common due to Tuberculosis infection.
Pulsion diverticula result due to pressure over the weakened esophageal wall, though it is unclear and the cause of such weakness is not certain. Epiphrenic diverticula are mostly of this type. Often they are seen with achalasia or after esophageal surgery.
EED is an uncommon presentation which develops secondary to increased esophageal pressure or motility disorder [2]. Besides achalasia, non-specific motility disorders and diffuse esophageal spasm might also be associated with ED [3,4]. They are false lesion without the muscular coating (Figure 1).
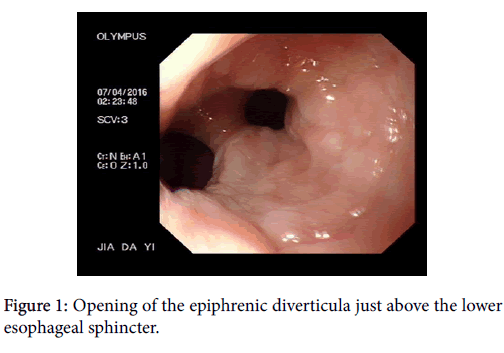
Figure 1: Opening of the epiphrenic diverticula just above the lower esophageal sphincter.
ZD is more symptomatic then EED as they cause localize swelling leading to pressure symptoms and compression like feeling [5]. Symptoms related to EED include chest pain, heartburn, vomiting, dysphagia, regurgitation and often lose weight in varying degrees. However, they can be completely asymptomatic and incidental findings, particularly in the small and shallow lesion. These symptoms are mostly because of the underlying cause rather than the diverticula itself [6]. Chest related symptoms like aspiration might be present in proximal esophageal diverticula whereas more distal lesion mostly presents as dysphagia to solid food. In the case of EED dysphagia may be progressive and severe but that associated with MD are usually intermittent [7]. Barium follow through is the most popular method of diagnosis, particularly in patients with multiple diverticula. CT scan is more useful for evaluation of postoperative and suspected traction lesions in the middle third of the oesophagus. However in all cases, upper GI endoscopy is essential for the treatment planning and evaluation of rare possibilities like malignancy or ulceration in the diverticula sac. Manometry is the key modality for patients with diverticula. In our patient initially, manometry was not performed because clinically the symptoms were diagnosed as a result of reflux esophagitis. As the post treatment follow-up showed significant improvement of the symptoms, the cause of EED in this particular case was uncertain (Figures 2 and 3).
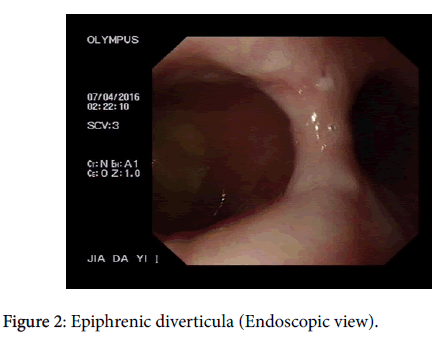
Figure 2: Epiphrenic diverticula (Endoscopic view).
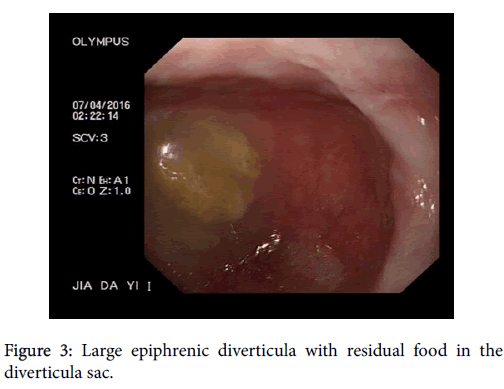
Figure 3: Large epiphrenic diverticula with residual food in the diverticula sac.
Treatment ED depends on the position, type and presenting symptoms of the disease. In case of asymptomatic lesions follow-up is recommended for a determination of the outcome. Symptomatic EED of >5 cm is an indication for surgery. Diverticula in the middle third of the oesophagus rarely require surgery. Treatment mostly requires for the underlying disease condition like achalasia [8]. Treatment for EED includes oesophageal myotomy, diverticulectomy, and fundoplication [3]. Minimally invasive surgery including laparoscopic surgery or video-assisted thoracoscopic surgery (VATS) has been used successfully for treatment of ED [9]. A case of long-standing diverticula might lead to stasis and overgrowth of bacteria causing inflammation. Such cases may lead to ulceration and might develop hemorrhage and perforation of the diverticula wall [10]. Besides this food particles also can be entrapped in the diverticula sac and create complications.
A large epiphrenic diverticulum is an uncommon presentation. The symptom of such condition mostly depends on the underlying pathology and disease process. Careful evaluation and clinical assessment are required for the successful treatment of disease conditions and recovery of symptoms.
Authors are grateful to all the professors and Doctors of Department of Digestive Disease-II, First affiliated Hospital of Jiamusi University for their generous support.