Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2015) Volume 4, Issue 3
Primary thyroid T-cell lymphoma is rare, with only 19 cases reported previously. T-cell prolymphocytic leukemia/ lymphoma (T-PLL) is a rare entity among T-cell lymphomas. T-PLL patients present with hepatosplenomegaly, lymphadenopathy, skin infiltration and a high leukocyte count, sometimes with anaemia and thrombocytopenia, but thyroid infiltration has been reported in only one other case. Here, we report an extremely rare case of T-PLL with foci seen in the thyroid gland and bone-marrow. Confirming the primary lesion was difficult, but the clinical and histopathological features suggest the thyroid gland as the primary lesion.
<Keywords: Hashimoto’s thyroiditis; Primary thyroid T-cell lymphoma; T-cell prolymphocytic leukemia/lymphoma
Malignant lymphoma of the thyroid gland is a rare entity, representing only 2-5% of all thyroid malignancies. These lymphomas are often associated with autoimmune diseases such as Hashimoto’s thyroiditis and Sjögren’s syndrome [1]. Malignant lymphoma associated with chronic inflammation (e.g., pyothorax-associated lymphoma or large B-cell lymphoma around the joints of rheumatoid arthritis patient) usually show B-cell characteristics. Similarly, lymphoma occurring in the thyroid also tends to show B-cell characteristics. T-cell lymphoma in the thyroid gland is thus extremely rare and we have only been able to identify 19 cases reported previously [2-19]. T-cell prolymphocytic leukemia/lymphoma (T-PLL) is a rare entity among T-cell lymphomas, representing only 0.06% of all malignant lymphomas according to data compiled by Japanese pathologists [20]. We report herein a rare case of T-PLL in which the primary lesion was suggested to be in the thyroid gland.
A 77-year-old woman came to our hospital for treatment of left breast cancer. Her history included Hashimoto’s thyroiditis with thyroid enlargement, diabetic mellitus, chronic hepatitis B, left cerebellar infarction and paroxysmal atrial fibrillation. Thyroid enlargement had been existed at least for 5 years though it is incorrect because the patient was followed up for thyroid disease at other institution. The patient told she was taking medicine for hypothyroidism before, but at the time of visit she was taking nothing for it.
Preoperative examination of breast cancer showed leukocytosis (White blood cell: 44,700/μL; normal, 4,800-9800/μL). During the checkup for leukocytosis, marked elevated level of soluble interleukin-2 receptor (sIL-2R) was revealed (sIL-2R: 2516 U/mL; normal, 122-496 U/ mL). Atypical lymphocytes represented a large proportion of peripheral white blood cells (87.5%). Mild anaemia was identified (haemoglobin, 11.1 g/dL; normal, 12.0-16.0 g/dL), but platelet level remained within the normal range. Serology for human T-cell lymphoma virus type 1 (HTLV-1) yielded negative result and C-reactive protein level was not elevated. Hypothyroidism was also seen (free T4: 0.5 ng/dL; normal, 0.7-1.7 ng/dL; free T3: 2.0 pg/mL; normal, 2.3-4.1 pg/mL; thyroid-stimulating-hormone: 57.64 μg/mL; normal 0.50-4.30 μg/ml). Thyroglobulin was elevated beyond the measurement range (>=1000 ng/mL), with elevated levels of anti-thyroglobulin antibody (52.1 IU/ mL; normal, 0.0-16 IU/mL).
Partial mastectomy of breast cancer had been done at first and the patient was followed at outpatient department. Since her first visit to our hospital, her thyroid gland started to show rapid additional enlargement. Computed tomography and echographic image showed diffuse enlargement of the thyroid gland. Thyroid scintigraphy showed decreased uptake of technetium-99m, and gallium scintigraphy showed diffuse accumulation of gallium-67 to the enlarged thyroid gland (Figure 1). Differentiating neoplasm from inflammation was difficult. No other lesions were identified, so thyroid gland incision biopsy was performed to make a diagnosis.
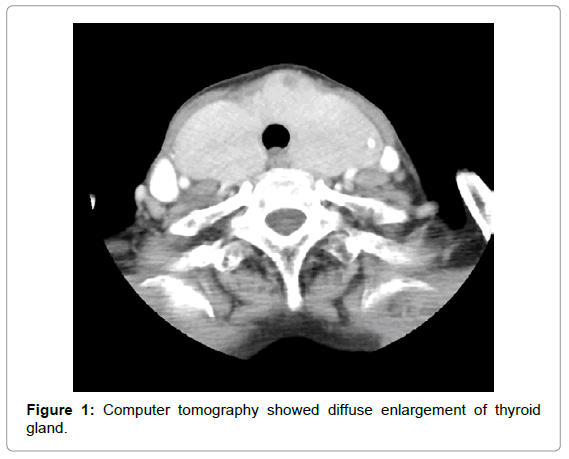
Figure 1: Computer tomography showed diffuse enlargement of thyroid gland.
The diagnosis of primary thyroid T-cell lymphoma was done and four cycles of leverage daily-etoposide was given after a cycle of combination of cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP) because the patient had gastrointestinal symptom with CHOP. The serum level of sIL-2R level is decreasing though it is still high (1788 U/mL; normal, 122-496 U/mL). Also the size of the tumor is getting smaller slightly but still enlarged. Hypothyroidism is treated by replacement therapy. Now she is followed up as an outpatient.
Peripheral blood films showed small to medium-sized atypical lymphocytes with non-granular basophilic cytoplasm and round, oval nuclei with visible nucleoli. Some nuclei had irregular contour and even showed a cerebriform shape (Figure 2).
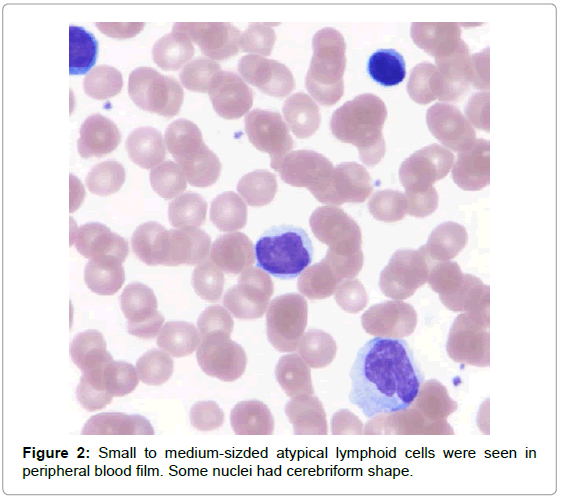
Figure 2: Small to medium-sizded atypical lymphoid cells were seen in peripheral blood film. Some nuclei had cerebriform shape.
Bone-marrow aspiration showed mild hypercellularity. Lymphocyte nests comprised small to medium-sized lymphocytes with round to slightly irregular contours. Other blood cell lineages were decreased (Figure 3). Atypical lymphocytes were positive for CD3, CD4, CD5, CD8 and CD45. CD3 staining was diffuse, but weak. On the other hand, terminal deoxynucleotidyl transferase (TdT), cyclinD1, CD10, CD23, CD34 and CD56 immunostaining showed negative results. Few cells showed positive immunostaining for CD20, CD79a and granzyme B (Table 1).
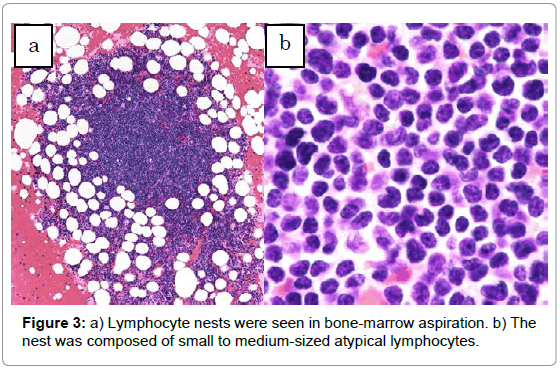
Figure 3: a) Lymphocyte nests were seen in bone-marrow aspiration. b) The nest was composed of small to medium-sized atypical lymphocytes.
| Bone-marrow | Thyroid gland | |
|---|---|---|
| CD3 | (+)(diffuse, weak) | (+) |
| CD4 | (+) | (+) |
| CD5 | (+) | (+) |
| CD8 | (+) | (+) |
| CD10 | (-) | (-) |
| CD20 | (+)(sporadic) | (-) |
| CD23 | (-) | (-) |
| CD34 | (-) | (-) |
| CD45 | (+) | (+) |
| CD56 | (-) | (-) |
| CD79a | (+)(sporadic) | (+)(sporadic) |
| TdT | (-) | (-) |
| GranzymeB | (+)(sporadic) | (+)(sporadic) |
| CyclinD1 | (-) | (-) |
| Thyroglobulin | (-) | (-) |
Table 1: Pattern of immunohistochemistry.
Thyroid gland specimens showed severe, diffuse infiltration of atypical lymphocytes among atrophic, eosinophilic thyroid follicles without a nodular pattern. Marked proliferation of endothelial venules was also evident. Diffusely infiltrated atypical lymphocytes were relatively uniform, small to medium-sized, round cells with a high nuclear-cytoplasmic ratio. These cells displayed round nuclei with increased coarse chromatin and small nucleoli. The atypical lymphocytes were positive for CD3, CD4, CD5, CD8 and CD45, but negative for TdT, cyclin D1, CD10, CD20, CD23, CD34, CD56 and thyroglobulin. CD79a and granzyme B immunostaining showed focal positive staining. The atrophic thyroid epithelia showed enlarged, eosinophilic granular cytoplasm with large nuclei, as so-called Hürthle cell metaplasia. These findings suggested a complication of long-term Hashimoto’s thyroiditis, although neither plasma cells nor eosinophils were seen at this point, probably due to invasion of atypical lymphocytes (Figure 4).
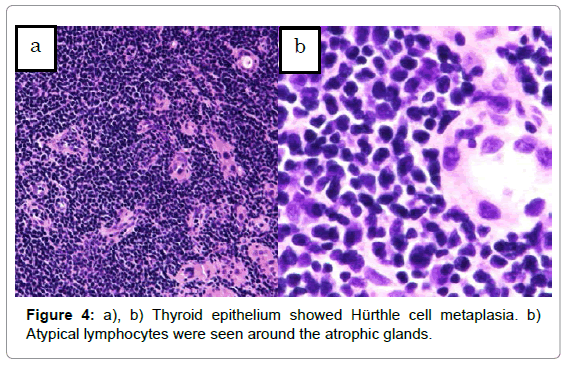
Figure 4: a), b) Thyroid epithelium showed Hürthle cell metaplasia. b) Atypical lymphocytes were seen around the atrophic glands.
Atypical lymphocytes were seen both in peripheral blood and bone marrow. Morphological and immunostaining characteristics of atypical lymphocytes suggested T-cell leukemia, potentially including T-PLL, adult T-cell leukemia/lymphoma and Sézary syndrome. Nuclear contours were irregular and some of those were slightly convoluted. Serological examination for HTLV-1 yielded negative result and the clinical course had included neither cutaneous symptom nor adenopathy. T-PLL therefore seemed the most likely diagnosis. In addition, the thyroid specimen showed a similar appearance and immunostaining pattern to bone marrow.
Surface marker analysis of freshly obtained peripheral blood showed T-cell dominance (CD2+, CD3+, CD4+, CD5+, CD7+).
Examination of the G-band pattern of the bone-marrow karyotype revealed no chromosomal abnormalities, but polymerase chain reaction showed rearrangement of T-cell receptor γ and β chains.
In this case, T-PLL was seen in only two lesions, in the bone marrow and thyroid gland. Determining which was the primary lesion proved difficult. However, the patient displayed characteristic clinical features of primary thyroid lymphoma [1], such as her age, sex, history of Hashimoto’s thyroiditis and rapid thyroid mass enlargement. From these points, we concluded that this case was consistent with primary thyroid T-PLL.
Only a previous report, posted by Fujiwara et al., has described thyroid gland infiltration by T-PLL [19]. In that case, the patient was diagnosed with T-PLL first from bone marrow, and subsequently in the thyroid gland. The authors therefore concluded that the thyroid lesion represented secondary infiltration, but they also noted that her clinical features such as history of Hashimoto’s thyroiditis and rapid enlargement of the thyroid gland were similar to those in primary thyroid lymphoma. We noticed further similarities between Fujiwara’s case and our own, and suspect that their case might also have represented primary thyroid T-PLL. In fact neither case showed splenomegaly nor skin infiltration, even though these symptoms are common in T-PLL. In addition both seemed to show a better prognosis than usual for T-PLL patients, with Fujiwara et al. describing survival for 15 months after diagnosis and death due to major stroke rather than lymphoma. As of the time of writing, our patient has survived 11 months since diagnosis, whereas the median survival after diagnosis of T-PLL is 6.5-7.5 months. This coincides with the fact that other primary thyroid T-cell lymphomas tend to show better prognosis than T-cell lymphoma occurred in other place [2-18]. Based on these atypical points in common, we propose a hypothesis that T-PLL associated with Hashimoto’s thyroiditis may show a clinical course different from usual for T-PLL.
To the best of our knowledge, this is the first report of a suspected primary thyroid T-PLL. To remind rare diagnosis pattern in thyroid gland here we reported this case. Further investigations are needed to clarify this matter.
The authors have declared no conflicts of interest.